Key Takeaways
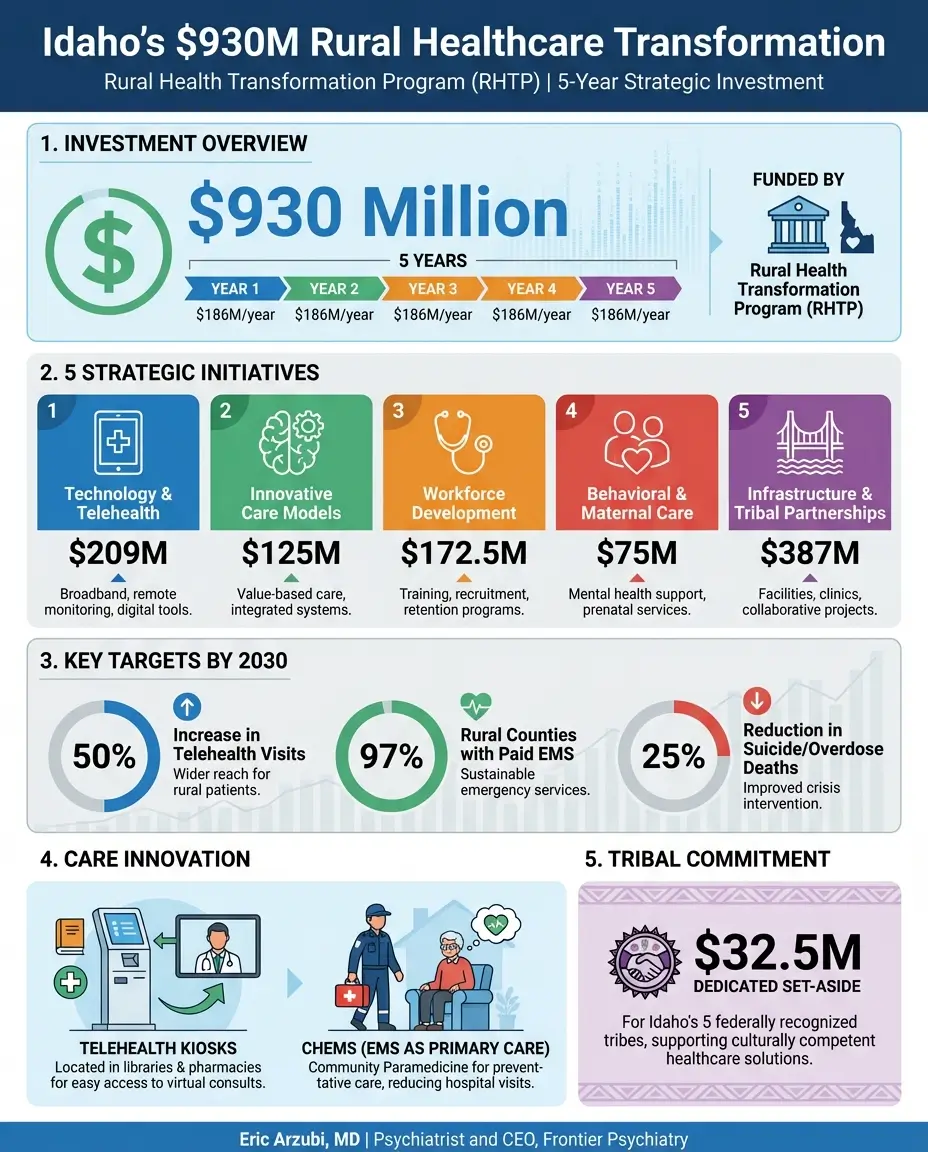
- The federal government is investing $930 million over five years to transform rural healthcare across Idaho, averaging $186 million per year through the Rural Health Transformation Program.
- Telehealth kiosks and diagnostic pods will be placed in libraries, pharmacies, schools, and community centers so rural residents can access care without long drives.
- EMS responders will be trained to deliver routine primary care, wellness checks, and chronic disease management in patients' homes, with 97% of rural counties gaining a full-time paid EMS position by 2030.
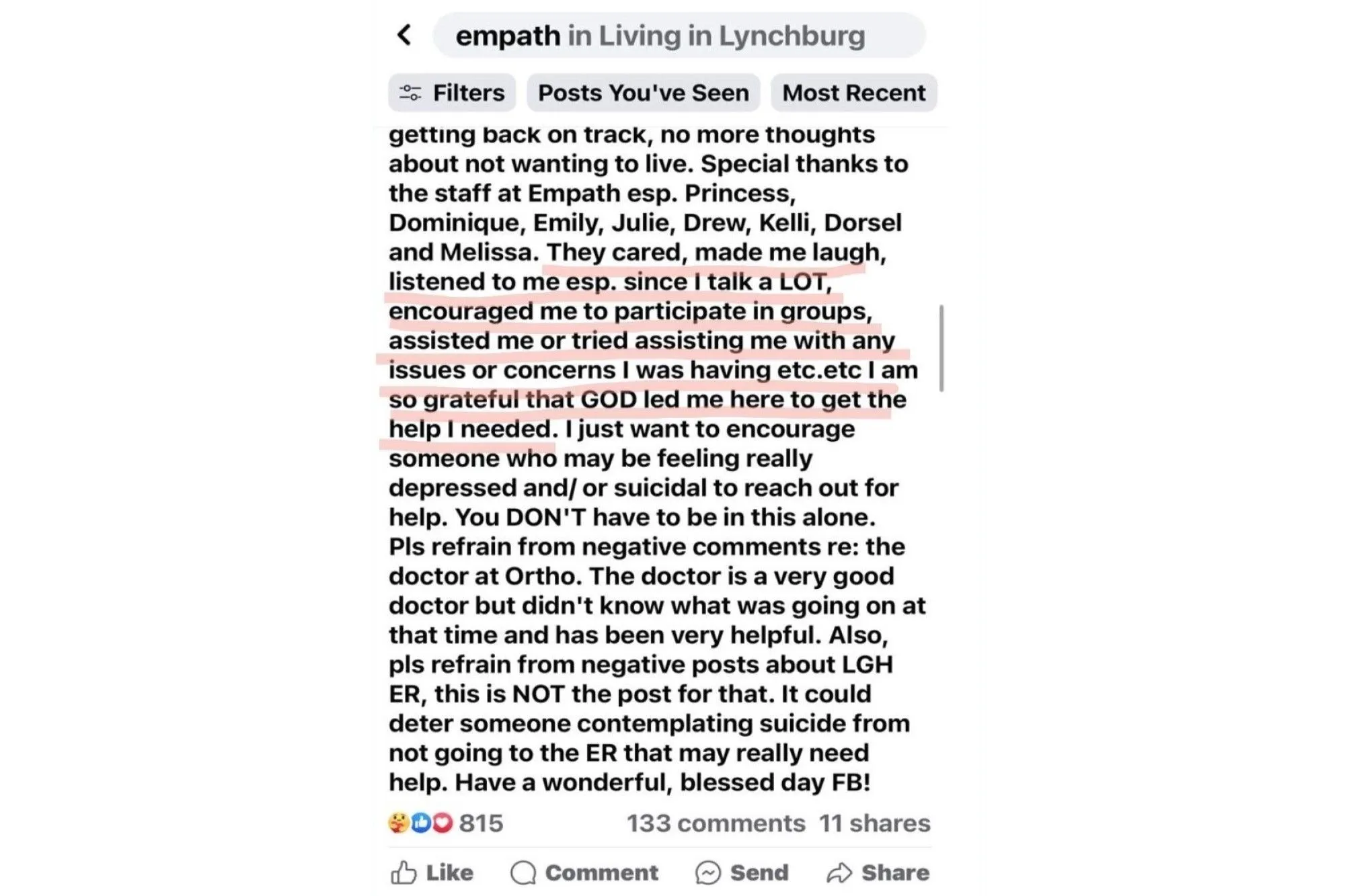
- Mental health crisis teams, a pediatric psychiatry access line, and school-based counseling access aim to cut deaths from suicide, overdose, and alcoholism by 25% by 2030.
- Idaho's five federally recognized Native nations will receive a dedicated $32.5 million set-aside to develop their own tribal healthcare transformation plans.
Idaho's $930M Rural Healthcare Transformation: What Providers and Patients Need to Know
The federal government announced a $930 million investment on December 30, 2025, to transform rural healthcare access in Idaho over five years. Led by the Idaho Department of Health and Welfare (IDHW), the plan includes telehealth kiosks in community spaces, EMS primary care training, mental health crisis teams, and $32.5 million for tribal healthcare partnerships, all funded through the Rural Health Transformation Program (RHTP) established under the One Big Beautiful Bill.
For a state where 100% of the land area is designated a Mental Health Health Professional Shortage Area and 46% of Critical Access Hospitals operate in the red, this is a landmark moment for rural healthcare in Idaho.
What's in the $930M Federal Investment?
The funding flows through the Centers for Medicare and Medicaid Services (CMS) at roughly $186 million per year over five years, organized around five major initiatives. Each one targets a different piece of Idaho's rural healthcare puzzle, with specific dollar amounts, measurable goals, and a built-in sunset plan so no initiative depends on permanent federal funding.
Here's how the money breaks down:
- Initiative 1, Technology and Telehealth Infrastructure: $209 million over five years to modernize how rural facilities deliver care, from EHR upgrades and cybersecurity protections to telehealth equipment and AI-driven clinical tools.
- Initiative 2, Innovative Care Models: $125 million to put diagnostic kiosks, telehealth pods, and pharmacy access points in everyday community locations, and to train EMS providers to deliver routine primary care.
- Initiative 3, Workforce Development: $172.5 million for recruitment bonuses, retention incentives, medical education scholarships, new residency and fellowship programs, and "grow your own" workforce pipelines in rural communities.
- Initiative 4, Chronic Disease, Behavioral Health, and Maternal Care: $75 million for evidence-based prevention programs, a pediatric psychiatry access line, mobile crisis response teams, and expanded perinatal quality initiatives.
- Initiative 5, Infrastructure and Tribal Partnerships: $387 million for facility renovations, clinical equipment purchases, mobile health units, safety code compliance, pharmacy solutions, and a dedicated 3.5% set-aside for Idaho's five federally recognized Native nations.
The plan's overall vision is rooted in the Make America Healthy Again (MAHA) framework, emphasizing prevention, personal responsibility, local control, and community self-sufficiency rather than permanent government expansion.
Telehealth Kiosks: Bringing Care to Libraries and Pharmacies
If you live in rural Idaho, there's a good chance the nearest specialist is a two-hour drive across mountain terrain. That's about to change.
A major piece of the plan puts diagnostic kiosks, telehealth pods, and care stations in the places rural Idahoans already go: libraries, pharmacies, schools, grocery stores, houses of worship, and community centers. These aren't stripped-down video screens. They're designed to support preventive screenings, lab testing, virtual consultations with specialists, and even remote patient monitoring for people managing chronic conditions at home.
The state will also install pharmacy kiosks and prescription lockers in community spaces and expand mail-order pharmacy services so patients can pick up medications without driving to the nearest town with a pharmacy.
On the backend, Idaho is investing in the infrastructure that makes all of this work. That means upgraded Electronic Health Records across rural facilities, new cybersecurity protections to keep patient data safe, AI-powered clinical tools for diagnostic support and risk stratification, and a modernized Health Alert Network to connect physicians across the state during public health emergencies. The target is to connect at least 80% of physicians in rural counties to the new Health Alert Network by December 2030.
The overarching goal: increase the number of telehealth and remote appointments by 50% by December 2030. For a state where 98.2% of the land is a Primary Care Health Professional Shortage Area and 95.01% is a Dental Health Professional Shortage Area, virtual care isn't a luxury. It's a lifeline.
Idaho was already an early adopter of telehealth. The Idaho Virtual Care Access Act established Medicaid reimbursement at parity with in-person visits, and the state doesn't require in-state licensure for remote providers who are licensed elsewhere and in good standing. This new investment builds on that foundation rather than starting from scratch.
Training EMS Responders as Primary Care Providers
Here's a statistic that explains a lot about rural Idaho: 69% of the state's rural EMS providers are volunteers. That's not a sustainable workforce.
The RHTP addresses this head-on with one of its most innovative strategies: transforming EMS personnel from emergency-only responders into Community Health Emergency Medical Services (CHEMS) providers who deliver preventive visits, wellness assessments, follow-up checks, and chronic disease management in patients' homes.
Right now, only 26 CHEMS positions support Idaho's rural counties, and just 28% of rural counties (13 of 43) have even one full-time paid EMS position. The plan sets an ambitious target: grow CHEMS positions to at least 62 by 2030, and ensure 97% of rural counties (42 of 43) have at least one county-level full-time paid EMS position.
This isn't just about emergencies. When a trained CHEMS provider visits a patient at home after a hospital discharge, checks their vitals, reviews their medications, and connects them to follow-up care, that prevents the next 911 call. The state is targeting a 20% reduction in emergency department visits for conditions that should be managed outside the ER, from roughly 30,779 per 100,000 ED visits in 2025 to less than 24,623 by 2030. Idaho also aims to reduce repeat EMS emergency responses (patients using emergency services more than once a year) from 32% down to 10% or less.
To make this sustainable, EMS agencies that receive funding will be required to create a sustainability plan for continuing these positions through alternative funding after year five. Staff must commit to five years of service in the rural area. Agencies will also participate in a statewide CHEMS workgroup with hospitals, clinics, payers, and state agencies to build long-term viability.
Idaho already supports expanded scope of practice for EMS personnel at all levels, including work in non-traditional settings like emergency departments. That legal framework makes the CHEMS expansion possible without waiting for new legislation.
Mental Health Crisis Teams: The 25% Reduction Goal
Idaho has the fourth-highest suicide rate in the nation. In rural counties, the rate is 28.6 deaths per 100,000 people. In the most remote counties, it climbs to 38.7 per 100,000, nearly double the state's urban rate of 21.0.
Meanwhile, 100% of Idaho's land area and population falls within a Mental Health Health Professional Shortage Area. Every single county. There is a complete statewide shortage of mental health professionals.
The plan attacks this crisis from multiple angles. It includes mobile crisis response teams that go to people in crisis rather than waiting for them to find their way to a clinic that may not exist. These teams will also provide post-crisis linkage, connecting individuals to ongoing care, including medication-assisted treatment (MAT) for substance use disorders. Mobile medication services will reach underserved areas to reduce overdose deaths.
For children, the plan funds a Pediatric Psychiatry Access Line (PPAL), a centralized resource that lets pediatricians consult directly with child psychiatrists about behavioral health conditions. Idaho currently has no such resource, which means pediatricians in rural areas are often managing complex mental health cases alone. The PPAL empowers them to identify and treat youth mental health conditions earlier and reduce unnecessary hospitalizations.
The plan also creates space within existing schools for parent-selected behavioral health professionals to see students during the school day, so rural families don't have to drive hours for a child's therapy appointment. All activities will follow Idaho's Parental Rights Act (Idaho Code 32-1010).
Community-based prevention programming will partner with healthcare facilities, community organizations, and faith-based groups to implement evidence-based mental health and substance use prevention efforts, with a focus on models that can sustain themselves after federal funding ends.
The targets: reduce deaths from suicide, drug overdose, and alcoholism by 25%, from 1,216 deaths in 2023 to 912 or fewer by December 2030. Monthly emergency department visits for these conditions should drop from 625 (September 2025 baseline) to 400 or fewer.
Tribal Healthcare: $32.5M for Native Communities
Idaho is home to five federally recognized Native nations, and the plan sets aside 3.5% of the total award, approximately $32.5 million, specifically for tribal healthcare transformation. That percentage is based on the American Indian population in Idaho relative to the total rural population, calculated using the most recent U.S. Census data.
This isn't a top-down allocation. IDHW will request the five tribes to submit a coordinated proposal for how to use the set-aside over the five-year period. That proposal is due by February 28, 2026. It must align with Idaho's overall RHTP plan and approved uses of funds, but the tribes themselves will determine their priorities.
The state conducted two formal Tribal Consultations with tribal leaders and held several additional meetings with tribal health leaders during the planning process. Those consultations gathered input on tribal member healthcare concerns, challenges, and specific needs for transforming care.
The goal: each of the five federally recognized tribes in Idaho will implement an approved RHTP plan aligned with the state plan by December 2030.
Given that Idaho's tribal communities face some of the most severe healthcare access challenges in the state, compounded by geographic isolation, workforce shortages, and historical underfunding, this dedicated investment represents a meaningful commitment to closing long-standing gaps.
How to Access These Resources
The RHTP funds will flow through IDHW to healthcare facilities, provider organizations, educational institutions, EMS agencies, and community partners through a formal subaward process. Here's what prospective applicants need to know.
Who's eligible: Rural healthcare facilities including Critical Access Hospitals (CAHs), Rural Health Clinics (RHCs), Federally Qualified Health Centers (FQHCs), EMS agencies, behavioral health providers, educational institutions, community-based organizations (including faith-based entities and houses of worship), pharmacies, and the five federally recognized Native nations in Idaho. The target population includes 655,070 residents in rural census tracts, with specific focus on pregnant and postpartum women, children and young adults under 20, older adults, and people with disabilities or medically complex conditions.
How funds will be distributed: IDHW will follow Idaho procurement and contracting laws along with federal requirements from the Notice of Funding Opportunity (NoFO). Subaward solicitations will include criteria such as full pricing transparency to patients, rural access guarantees, long-term fiscal discipline and sustainability planning, alignment with target populations, feasibility within the funding period, and direct health impact on rural Idahoans. All subawards must demonstrate that funded activities are new or newly expanded into rural communities, not duplications of existing programs.
Key contacts: IDHW is the lead agency. A Governor's RHTP Task Force, including legislators from rural districts, State Board of Education members, Workforce Development Council representatives, Idaho Military Division, tribal government leaders, and IDHW staff (including the State Medicaid Director and Office of Rural Health), provides oversight and guidance.
Important dates: Contracts and partnerships begin executing in Q1-Q2 of 2026. Statewide assessments launch concurrently. Most programs begin rolling out in 2027, with full-scale implementation by 2028-2029. Tribal proposals are due February 28, 2026.
What to prepare now: If you're a rural provider, start documenting your technology gaps, workforce needs, and facility condition. The state will conduct technology readiness assessments, community needs assessments, and financial viability assessments. Having your data ready will position you to access funds early.
Timeline: What Changes When
2026, Foundation Year. Contracts executed. Statewide assessments of technology, workforce, and facility needs completed. Program infrastructure built. Tribal proposals submitted and reviewed. Cybersecurity baseline assessments finished. Curriculum developed for health extender certification programs. First pilot recruitment and career exploration programs launch. IDHW hires 15 dedicated staff.
2027, Launch Year. Telehealth equipment installed at first rural sites. Diagnostic kiosks and telehealth pods go live in pilot communities. First cohort of health extenders deployed. EMS support grants disbursed to high-need counties. Recruitment incentives and scholarships activated. Residency and fellowship programs begin training. Mobile health units and transport vehicles deployed. Pharmacy upgrades and locker installations begin. First facility renovation grants awarded.
2028, Scale Year. Regional telehealth networks operational. Remote patient monitoring integrated with local clinics. Pharmacy lockers and mail-order services expanded. AI tools for revenue and care optimization deployed in pilot facilities. Chronic disease and behavioral health programs expand enrollment. Graduate medical education programs active in rural settings. Emergency communication systems upgraded to Next Generation 911 standards.
2029, Evaluation Year. Midpoint evaluation reports across all initiatives. Programs refined based on outcomes data. Sustainability planning intensifies. Regional analytics dashboards deployed. Multi-facility EHR interoperability achieved. Two-year retention bonuses disbursed to early workforce cohorts.
2030, Target Year. 97% of rural counties with paid EMS. 50% increase in telehealth appointments. 25% reduction in deaths from suicide, overdose, and alcoholism. 20% reduction in preventable ED visits. 90% patient satisfaction on "getting needed care." At least 200 individuals complete "grow your own" workforce programs. Eight rural hospitals complete new perinatal collaborative initiatives.
2031, Close-Out Year. Final evaluation and impact reporting. Successful models transitioned to long-term local ownership and sustainable funding streams. Technology systems handed off to permanent management. Results disseminated to state policymakers and stakeholders.
What This Means for Idaho's Healthcare Future
For providers, this investment changes the math. Rural facilities operating on razor-thin margins (remember, 46% of Idaho's Critical Access Hospitals currently operate in the red, with one already converting to a Rural Emergency Hospital just to stay viable) will get the technology upgrades, workforce support, and infrastructure improvements they need to stay open and expand services. New reimbursement pathways, better billing systems through AI-powered revenue cycle management, and shared infrastructure costs should improve financial sustainability beyond the five-year funding window.
For patients, the change is more personal. It means a grandmother in a frontier county can get a diabetes check at the local library instead of driving 90 minutes to a clinic. It means a teenager struggling with depression can see a counselor at school instead of missing a full day of classes. It means a volunteer EMS crew in a county with fewer than six people per square mile gets a full-time paid colleague who can do wellness visits, not just emergency runs.
Idaho designed this plan to avoid creating permanent government dependency. Every initiative includes sustainability milestones, graduated funding scale-downs, and requirements for local ownership by year five. Projects that fund personnel or operating costs follow a graduated scale-down model, reducing dependency each year so that by year five, local partners and health systems are positioned to sustain operations independently through new reimbursement streams, local partnerships, and demonstrated efficiency gains.
Whether the plan delivers on its ambitious targets depends on execution. But with $930 million, five years, and a clear set of measurable goals, rural Idaho has a real shot at building a healthcare system that works for the people who need it most.
Frequently Asked Questions
How much funding is Idaho receiving for rural healthcare?
Idaho is receiving approximately $930 million over five years through the federal Rural Health Transformation Program (RHTP), averaging roughly $186 million per year. The funding comes through the Centers for Medicare and Medicaid Services (CMS) under the U.S. Department of Health and Human Services.
What are telehealth kiosks and where will they be located?
Telehealth kiosks are technology stations that allow patients to conduct virtual visits, preventive screenings, and lab testing. They will be placed in libraries, pharmacies, schools, grocery stores, houses of worship, and community centers across rural Idaho.
How will EMS responders provide primary care?
Through the Community Health Emergency Medical Services (CHEMS) model, trained EMS professionals will conduct preventive visits, follow-up checks, wellness assessments, and chronic disease management in patients' homes, expanding their role beyond emergency response.
What is the goal for mental health crisis response?
Idaho aims to reduce deaths from suicide, drug overdose, and alcoholism by 25% by December 2030, from 1,216 deaths in 2023 to 912 or fewer. Monthly emergency department visits for these conditions should drop from 625 to 400 or fewer.
How much funding goes to tribal healthcare?
A 3.5% set-aside of the total award, approximately $32.5 million, is dedicated to healthcare transformation for Idaho's five federally recognized Native nations. Tribal proposals for use of these funds are due February 28, 2026.
Who is eligible for these healthcare resources?
Rural healthcare facilities (CAHs, RHCs, FQHCs), EMS agencies, behavioral health providers, educational institutions, community organizations (including faith-based entities), pharmacies, and Idaho's five federally recognized Native nations. The target population is 655,070 rural residents, with emphasis on pregnant women, children under 20, older adults, and people with disabilities or medically complex conditions.
When will these changes take effect?
Contracts and assessments begin in early 2026. Most programs launch in 2027, reach full scale by 2028-2029, and hit target outcomes by December 2030. Final evaluation and close-out occur in 2031.
Sources
- Idaho Department of Health and Welfare, Rural Health Transformation Program Project Narrative (CMS-RHT-26-001), submitted 2025.
- U.S. Census Bureau, ACS 5-Year Estimates, Table DP05 (2023). Idaho population and demographic data.
- Health Resources and Services Administration (HRSA), State of the Primary Care Workforce, 2024.
- Rural Health Information Hub, Idaho state profile (2024). HPSA designations and rural healthcare facility data.
- Idaho Department of Health and Welfare, Get Healthy Idaho, statewide health assessment.
- The Chartis Group, 2025 assessment of Idaho Critical Access Hospital financial vulnerability (contract deliverable for IDHW).
- Idaho Center for Nursing, 2024 Report on Idaho Nursing Workforce.
- Kozhimannil, K. B., Interrante, J. D., & Thao, V. (2024). Obstetric Care Access Continues to Decline at Rural and Urban Hospitals. Maternal and Child Health Journal, 28(8), 1709-1717.
- U.S. Census Bureau, Health Insurance Coverage by State: 2023 and 2024 (Report No. ACSBR-024).
Eric Arzubi, MD is a board-certified psychiatrist, CEO and Co-Founder of Frontier Psychiatry, and Assistant Clinical Professor at the Yale Child Study Center. Frontier Psychiatry provides telehealth behavioral health services across Montana, Idaho, and Alaska, serving approximately 6,000 active patients through research-backed care that published in JAMA Network Open demonstrated 38% lower hospitalization rates compared to standard care. Dr. Arzubi is America's #1-ranked LinkedIn mental health voice and author of "From Silence to Solutions."